“This just in: Apparently, there is more than one
connection between all of the previous rampage killers in the US. Not only did
they all play violent video games at some point, they all watched TV news AND
had access to guns.”
While the above discussion is obviously fake, according to
footage in the Colbert
Report of September 18, 2013 one TV journalist has suggested that we
could perhaps prevent future firearm violence by keeping a register of video
game purchases.
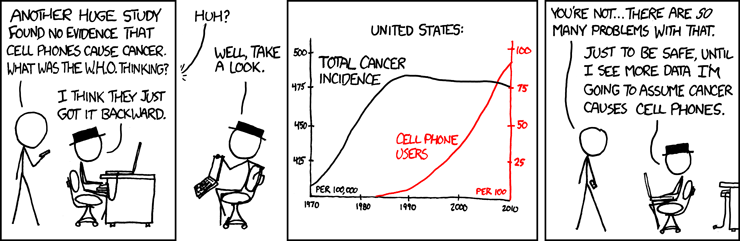 |
| xkcd on reverse causation |
How did the discussion of what is behind these
horrible shooting rampages end up being about video games? Simple:
As a society, we
want to understand what caused this so we can prevent it in the
future.
As another
video game researcher puts it,
“We don't have a lot of control over many of the factors
that can contribute to violent behavior. But we have some control over violent
video games. We can make it more difficult to get access to them. We can
strengthen our laws against teens acquiring these games.”
Hold the phone; is he talking about video games or
guns? Let’s rewind and make a substitution:
“We don't have a lot of control over many of the factors
that can contribute to violent behavior. But we have some control over guns. We
can make it more difficult to get access to them. We can strengthen our laws
against teens acquiring these guns.”
Everyone knows that you can’t have firearm violence without
firearms. The cool thing about public health is that
- there
is (ideally) a scientific approach to understanding the processes that
lead to outcomes, and
- there
is also (ideally) an approach to deciding what is important to study and
regulate. One of the key questions to ask about a potential research
subject is: how much of an effect would being able to change
this potential cause have on my outcome of interest?
So, keeping in mind the important limitations of
public health research I discussed in my earlier posts, let’s talk about just a
couple of the reasons why keeping video games on the research and policy agenda
is a waste of time and resources:
1. Guns are clearly
responsible for firearm violence and can be regulated, even in other countries
that have traditionally refused limitations. (Take a look at the Emmy Award winning
segment of The Daily Show, where comedian John Oliver discusses the
complete absence of shooting rampages in Australia after gun control with
former Australian prime minister John Howard.)
2. Scientists have
been studying the effects of video games for decades, and there is still no
consistent relationship between violent video games and real-world violent
acts. In fact, one recent
well-controlled study showed no long-term ties between violent video
games (when measured by themselves) and real-world seriously violent acts when
other factors like substance use or living in a violent community are taken
into account (p.932; remember the previous discussion about statistical levels
and coincidence). It did show, however, that visiting websites that “feature
real people fighting, shooting or killing” is associated with real-world
violent acts. I’ll get back to more of the methodological problems in future
blog posts, but feel free to read anything by Chris
Ferguson or Craig
Anderson for more information and contrasting views on the research to
date.
3. Video games and
other media exposures are not proximal causes,
only distal links on a chain of other causes (see an excellent article by Krieger for
a thorough discussion). And contrary to the implication above, we
actually do have some control over the more proximal causes
(e.g, guns).
4. Multifinality and equifinality.
These limitations lead to different ways of viewing how likely or probable
something is (risk). And this little bit is going to be our public health
lesson for the day.
Multifinality: People can have the same risk
factors (potential causes of a bad event) but different outcomes.
Aaron Alexis and Adam Lanza both played video games (like
the majority
of people in the US). They also (probably) watched TV, were male, and
walked upright.
The above helps us understand questions about risk that are
vital to approaching things from a public health perspective. For the terms
below, I paraphrase a discussion by Swanson,
substituting “violent video games” for “mentally ill”.
Absolute risk: The vast majority of people who
play violent video games are not violent.
Relative risk: People who play violent video
games are no more likely to commit violent crimes than those who do not play
violent video games. (However, people who have access to guns are more
likely to shoot people.)
And then there’s equifinality: A variety
of risk factors can lead to the same outcome.
Aaron
Alexis was a former Naval reservist with a criminal history of
violence and current money troubles. He was also an African-American practicing
Buddhist who had sought help from the Veterans Administration for paranoia and
hearing voices. He had a legally-purchased
shotgun.
Adam Lanza was a well-off young white man who lived an
isolated life after years of being bullied in
high school. He also had access to a stockpile
of guns with over 1600 rounds of ammunition.
Attributable risk: Violence is a societal
problem caused largely by things other than violent video games (ready
availability of guns, for example).
The stories we hear about rampages are just that, stories.
They may serve the purpose of trying to make sense of something horrible, but
it’s time to move on from investing more time and money into studying video
games and consider what could provide “more bang for the
buck”. Some of the key assumptions of the Code
of Ethics for Public Health say that a base for action should improve
health through seeking and acting on knowledge, and that there is a moral
obligation to share what is known.
Yes, there are barriers to getting the knowledge out there
(e.g., publication bias, selective outcomes reporting). Yes, it is hard to take
action on things that we know (e.g., gun
control politics). But given that toddlers
with guns seem to have killed more Americans this year here in the US
than terrorists did, it’s time to take advantage of this window of opportunity
and enact real change in the clearest cause of firearm violence—access to guns.
reprinted from mcoldercarras.com, 9/2013
reprinted from mcoldercarras.com, 9/2013

